Why Strength Training for Women Over 35 is Important
What changes after 35, what happens to muscle, bone density and hormones and exactly how smart strength training helps you stay strong, lean, and capable.
If you’re a busy professional or a mum in Amstelveen or Amsterdam, strength training after 35 is one of the smartest “time-for-results” investments you can make. It protects the two tissues that naturally change with age, skeletal muscle and bone and supports posture, energy, insulin sensitivity, and confidence through perimenopause and beyond.
At NXT LVL, most women we coach aren’t trying to become bodybuilders. They want to feel strong, lean, pain-free, and capable: lifting kids without back pain, carrying luggage easily, feeling stable on stairs, and staying consistent even when life is hectic.
Want help applying this to your routine and lifestyle?

8 Week Longevity Program
Personal Training + Dietitian support: ideal for women 35+ who want structure, accountability, and measurable progress.

Reformer Pilates Group Classes
Great for core strength, posture, and mobility, especially when combined with strength training.

Personal Group Training (Functional Strength)
Weightlifting coaching + community + strength training.
What changes physiologically after 35 and why it happens
Muscle mass and sarcopenia risk
What changes. Across adulthood, skeletal muscle mass and strength tend to decline; commonly cited estimates indicate muscle mass decreases by roughly 3–8% per decade starting around age 30, with faster loss later in life. While “sarcopenia” is most often discussed in older adults, the underlying adverse muscle changes accrue over the lifespan, and earlier prevention is part of the logic of modern consensus definitions.
Why it happens. The drivers are multi-factorial:
– Neuromuscular aging: progressive loss of motor neurons and incomplete compensation by reinnervation contributes to fewer/smaller muscle fibers and declining function.
– Anabolic resistance: aging muscle becomes less responsive (on average) to anabolic stimuli like dietary protein and exercise, meaning you often need a stronger “signal” (adequate training stimulus and protein) to drive the same muscle-protein synthesis response.
– Activity and loading patterns: modern life often reduces regular high-tension loading (sprinting, lifting, climbing), and muscle is “use-it-or-lose-it” tissue.
Bone density, osteopenia, and osteoporosis risk
What changes. Bone mass peaks by about age 30 and then, especially around menopause, many women experience accelerated bone loss for several years. This matters because lower bone density increases fracture risk, and osteoporosis is both common and often silent until a fracture occurs.
Why it happens. Bone constantly remodels via osteoclast-mediated resorption and osteoblast-mediated formation. Estrogen plays an important regulatory role; when estrogen falls in menopause, remodeling can become imbalanced toward greater resorption (net loss). This is why menopause is widely recognized as a major accelerant of bone loss.
How fast can bone change? Rates vary widely. In cohort data tracking women through the menopausal transition and early postmenopause, average lumbar spine and femoral neck BMD declines were about 1.5% and 1.3% per year, respectively (with substantial individual variability). Patient-facing education from the Bone Health and Osteoporosis Foundation also notes that some women can lose up to ~20% of bone density in the five–seven years after menopause, underscoring how wide the range can be.
Hormonal shifts after 35: perimenopause, estrogen, testosterone, and insulin
Perimenopause basics. Perimenopause is characterized by increasingly irregular cycles driven by erratic ovarian hormone production and changes in ovulation frequency; many women first notice cycle changes in the 40s, though symptoms can begin earlier. A major theme is variability: estrogen and progesterone can fluctuate markedly before their eventual postmenopausal decline.
Testosterone and androgens. Unlike the sharp drop in ovarian estrogen at menopause, circulating testosterone shows a more gradual age-related pattern across midlife in population research, with declines observed from about age 40 to later midlife (and not necessarily a menopause-specific “cliff”). Practical implication: “hormones” are not the only lever, training and nutrition remain modifiable inputs that support muscle and function regardless of exact hormone trajectories.
Insulin and metabolic changes.During perimenopause, many women experience a shift toward more visceral (abdominal) adiposity even with modest weight change, which is clinically relevant because visceral fat is linked to cardiometabolic risk and insulin resistance. While hormone biology is complex, estrogen is repeatedly implicated in regulation of fat distribution and metabolic health, and menopausal transition is associated with higher metabolic risk at the population level.
How strength training improves these markers
Muscle and strength: improves neuromuscular efficiency and supports lean mass.
Bone density: progressive loading supports bone remodeling (especially hips and spine when programmed well).
Metabolic health: more muscle supports glucose management and energy stability.
Joint resilience: stronger tissues around joints improve tolerance for daily life (stairs, carrying, lifting kids).
Mood & stress: strength training is consistently linked to better mood and self-efficacy, crucial during hormonal transition.

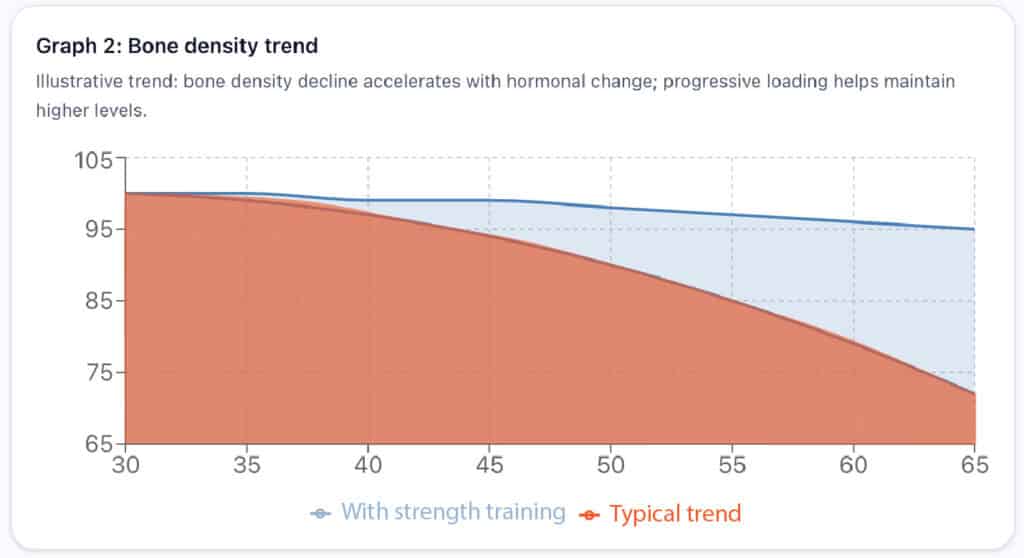
Illustration (not real patient data). Trends are simplified for education.
Strength training + Reformer Pilates: a powerful combo after 35
If you’re dealing with tight hips, back sensitivity, posture issues or you’re returning to training after a long break, combining 2 strength sessions/week with 1-2 Reformer Pilates class/week can be a sweet spot. Strength provides the muscle and bone stimulus; Reformer reinforces control, alignment, and core stability, especially helpful for women who sit a lot or carry daily stress.
In Amstelveen, you can join our Reformer Pilates group classes here.

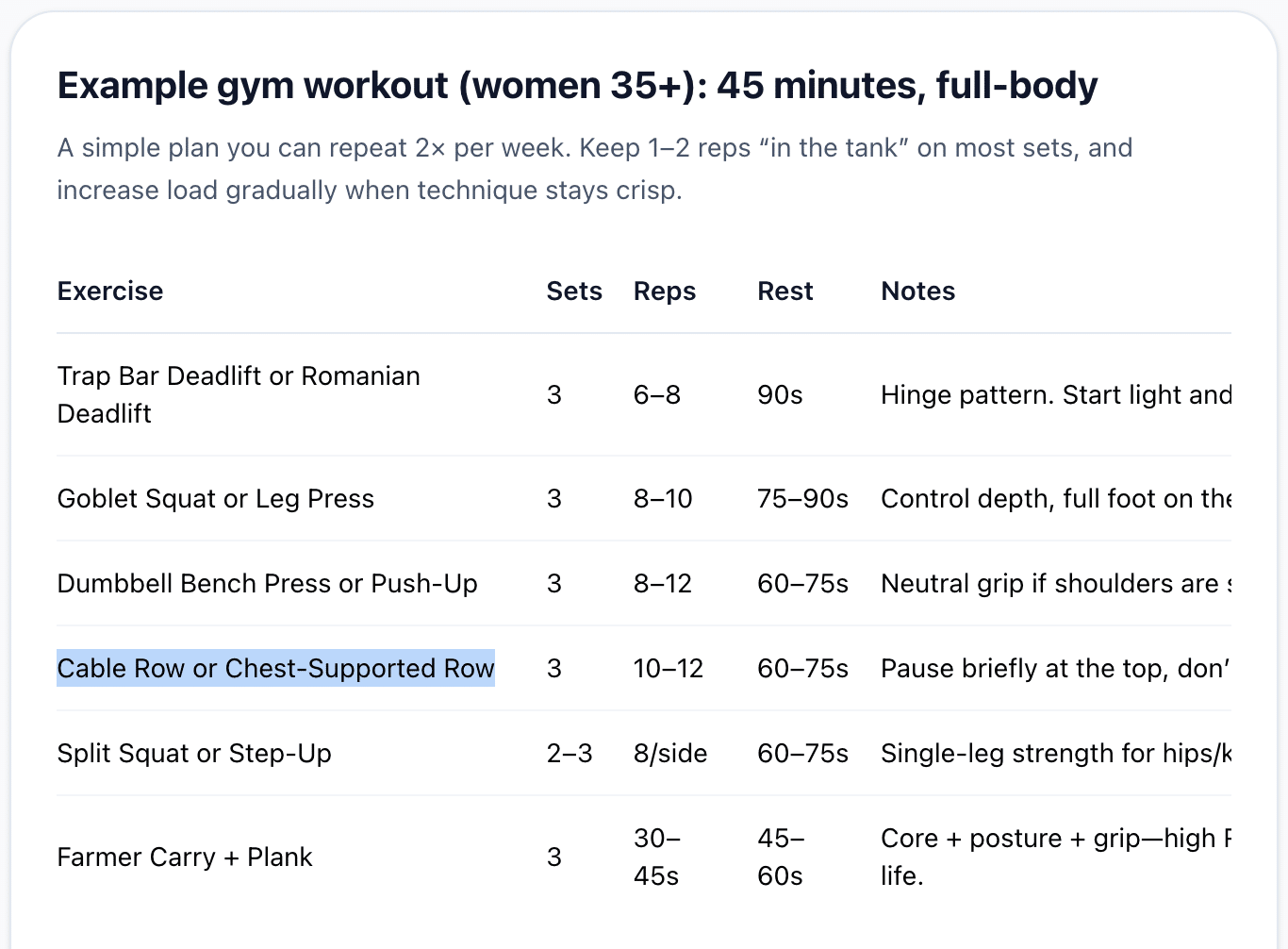
Example gym workout (women 35+): 45 minutes, full-body
A simple plan you can repeat 2× per week. Keep 1–2 reps “as reserve” on most sets, and increase load gradually when technique stays crisp.
{kind=link}
| Exercise | Sets | Reps | Rest | Remarks |
|---|---|---|---|---|
|
Trap Bar Deadlift or Romanian Deadlift |
3 | 6-8 | 90 sec |
Hinge pattern. Start light and master form. |
| Goblet Squat or Leg Press | 3 | 8-10 | 75-90 sec |
Control depth, full foot on the floor. |
|
Dumbbell Bench Press or Push-Up |
3 | 8-12 | 60–75 sec |
Neutral grip if shoulders are sensitive. |
| Cable Row or Chest-Supported Row | 3 | 10-12 | 60–75 sec |
Pause briefly at the back, don’t rush. |
| Split Squat or Step-Up | 2-3 | 8/side | 60–75 sec |
Single-leg strength for hips/knees stability. |
| Farmer Carry + Plank | 3 | 30-45 sec | 45-60 sec |
Core + posture + grip—high ROI for daily life. |
Strength training + Reformer Pilates: a powerful combo after 35
If you’re dealing with tight hips, back sensitivity, posture issues or you’re returning to training after a long break, combining 2 strength sessions/week with 1-2 Reformer Pilates class/week can be a sweet spot. Strength provides the muscle and bone stimulus; Reformer reinforces control, alignment, and core stability, especially helpful for women who sit a lot or carry daily stress.
In Amstelveen, you can join our Reformer Pilates group classes here.
FAQ: strength training for women over 35 (Amstelveen / Amsterdam)
Start with 2 full-body sessions per week. If recovery is good, move to 3 sessions. Consistency beats intensity.
For most women, yes, especially with good technique and a progressive plan. If sleep/stress is high, adjust training volume rather than stopping.
Beginners benefit most from coaching. Start with simple patterns (squat/hinge/push/pull/carry) and progress gradually.
If your goal is muscle, bone density, and metabolism, strength training should be the foundation. Reformer is a great add-on for control and posture. See our Reformer Pilates classes.
If you want structure and fast progress with minimal decision fatigue, a coached program is best, like our 8-week longevity program.
Yes, our Personal Group Training combines coaching, community, and progressive functional strength.